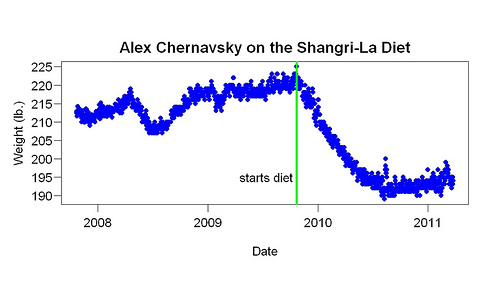
Alex Chernavsky has kindly given me several years of weight data he collected by weighing himself daily. He read about the Shangri-La Diet in 2005 and several years later decided to try it. The graph above shows what happened: Starting at 222 pounds (BMI = 32), over 11 months he lost 31 pounds, reaching a BMI of 27. Since then — while continuing the diet — his weight has increased at roughly the same rate it was increasing before he started the diet.
He started by drinking olive oil and sugar water, switched to olive oil alone, and then, finally, to flaxseed oil alone of which he drinks 3.5 tablespoons/day (= 420 calories/day). He does not clip his nose shut when he drinks it but he washes his mouth with water afterwards. More about his method here.
Almost all weight-control experts would say these results are impossible: 1. Alex lost weight because he ate more fat. Fat is fattening say most nutrition experts. 2. Atkins dieters, who don’t say that, think the secret of weight loss is to reduce carbohydrate. Alex didn’t do that (and eats plenty of carbohydrate). 3. He didn’t restrict what he ate in any way. 4. He didn’t change how much he exercised.
Quite apart from how it contradicts mainstream beliefs, including Atkins, the data are remarkable because the change was so simple, small, and sustainable, the weight loss so large, the rebound so minimal, and data period so long.
An ordinary clinical trial has obvious advantages over such one-person data, such as more subjects and more data per subject. Less obvious are the advantages of this sort of data over clinical trials:
1. Long pre-diet baseline. Clinical trials never have this. It allows one to judge if weight increase post-diet, often called “regain”, is due to the weight loss or other factors. In this case the rising pre-diet baseline shows that other factors are causing slow weight gain over time.
2. Motivation. In a clinical trial, the motivations of the researchers and the subjects are different. The researchers want to measure the effect of an intervention; the subjects want to lose weight. If paid, they may want to make money. The difference in motivations causes problems. How closely the subjects obey the researchers and how truthful they are is usually hard to know. This data does not have that clash of motivations and incentive to lie.
3. Realism — what methodologists call ecological validity. These data, unlike clinical trial data, come from the situation to which everyone wants to generalize: people trying a diet by themselves at home without professional support or guidance.
4. Level of detail available. You (the reader) have access to something resembling raw data. In clinical trial reports, the data available is heavily filtered (e.g., shortened, simplified) and the nature of the filtering rarely described. For example, you rarely learn in any detail what the subjects ate. With this sort of data, but not clinical trial data, you can get a better sense of whether the results are likely to apply to you.
That slow upward trend is a little worrisome to me. I think it might be caused (or exacerbated) by the fact that about eight months ago, I started eating breakfast two or three times per week (I still almost never eat lunch). I enjoy eating a home-cooked breakfast with my wife on weekends.
Alex, such slow upward trends are very common — and yours seems to have started at least as early as 2008. I think they are due to strengthening of food-calorie associations — what most people think of as “food becoming more familiar”. I came across a study that found that the thinner people are at age 20, the slower the weight gain in their 30s and 40s (comparing one culture to another).
It occurs to me that the obvious cofounding factor is that by taking on this ritual of dosing with oil and waiting to eat, a person may start to pay more attention to food intake and subsequently lose weight. In any event – good work, Alex!
Seth — you’ve mentioned nose-clipping. Anything else you might recommend to flatten or reverse that upward trend?
I was going to mention to you, and I guess this is as good of a place as any, that I’ve been noseclipping protein shakes in the morning (and rinsing as well. The flavor is very strong and sticks around without rinsing). I wasn’t sure about what kind of results I was getting, hunger-wise, until I, while lying in bed, realized that I could easily list everything I’d eaten that day. I got up, added up the calories, and it was about 1200. This is an unbelievable reduction, compared to before I started using your advice. I’m very pleased and impressed.
Thanks, Kevin. How long have you been doing this
Alex, no, no other suggestions. About noseclipping: I find it much easier to noseclip butter (with a little piece of meat) than ordinary food. I think that is because with ordinary food, noseclipping reduces how enjoyable it is. For example, a noseclipped sandwich is less pleasant than a sandwich eaten normally. Whereas with the butter, all of the pleasure is in the texture (which isn’t just fat, the protein helps). Noseclipping has no effect on that, so the nose-clipped butter is just as pleasant as the butter eaten normally. To be vegan about it, I’d eat the butter on a snap pea or a cracker.
I really enjoy my spelt toast with flax seed oil and ground flax on top (to absorb excess oil) in the morning, though I do it nose-clipped.
I found that toast with flaxseed oil eaten noseclipped tasted the same as toast with lots of butter.
I don’t noseclip, but I use a squirt bottle to bounce the oil off the back of my throat. In Berkeley, the ordinary Barlean’s brand comes in a squirt bottle, which I imagine has the extra advantage of minimizing oxygen exchange, so maintaining freshness. Of course any brand of oil can be put in a squirt bottle.
I wonder if the reason why Atkins works (for a while) is that meat without carbohydrates does not create as strong calorie-flavor association as it does with carbs. I personally do like meat, but a meal of only vegetables and meat does not create a genuine craving for me. Whereas high-calorie dinner with a good amount of carbohydrates does. People say it’s great that you can eat all the meat you want with Atkins diet, but I wonder if it is just not as satisfying.
This could explain why people find that even Atkins diet takes some self-discipline. They still crave for foods that have a lot of carbohydrates. Atkins is still to adhere to than the normal calorie-restriction diet, but it’s not automatic like Shangri-La diet is (when it works). This could also perhaps explain why many people can’t keep with their Atkins diet. (I don’t know the actual numbers, but I’ve understood that lapsing is somewhat of a problem with Atkins too.)
I found that my diet really switched around, but that at some point the food I was eating seems to have become too regularized. I’m now working on changing that.
Though if I go back to rigid eating, my weight drops again. I’m working out how to get away from rigidly eating a basically flavorless diet and how to deal with eating at restaurants and such on a regular basis.
I’m starting to consider just skipping lunch every day.
I start my SLD today
Over a year ago I weighed 85 kilos today I weigh 108 ks a cool 238 lbs.
9 months ago i gave up smoking (40 aday habit) and stopped working from Aid work: 18 warzones and more.
When I worked in Greece many greeks took 2 tbs of olive oil a day as laxative.
One question light olive boil is labelled ‘light and mild’ I assume its the same as in the US?
Thanks
Paul
I’ve been doing it for a couple of weeks in combination with a slow carb diet